Effect of 119 emergency medical services response time on return of spontaneous circulation
Author: HYEJI KWON PhD | Researcher | Hanyang University, Institute for Health and Society
Associate Authors: Young jeon, Shin,Hanyang University, School of Medicine, Graduate School of Public Health, Institute
Objective
This study evaluated the impact of emergency medical service (EMS) response time on prehospital return of spontaneous circulation (ROSC) in out-of-hospital cardiac arrest (OHCA) patients in Busan, South Korea.
Methods
.
We analyzed prehospital care and cardiac arrest reports from the Busan Fire and Disaster Headquarters between January and December 2022. To determine the optimal response time cutoff for predicting prehospital ROSC, we conducted a receiver operating characteristic (ROC) curve analysis using the Youden index. After excluding emergency medical service response time groups with fewer than 30 cases, multivariable logistic regression was performed on 2,268 cases. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
.
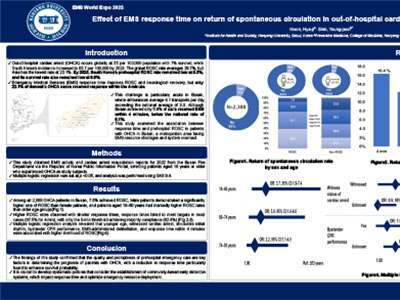
A total of 2,388 out-of-hospital cardiac arrest (OHCA) patients were identified in the Busan region, of whom 179 (7·5%) achieved return of spontaneous circulation (ROSC). Men comprised 63·7% of patients, and the age distribution showed the highest proportion (27·5%) in the 74-83 years age group. Cardiac arrest was unwitnessed in 53·7% of cases. Emergency medical services response times failed to meet the 4-minute benchmark in 97·5% of cases, and pharmacological interventions were not administered by emergency medical service provider in 96·2% of cases. ROC curve analysis showed limited predictive power of response time for prehospital ROSC (AUC = 0.53). The optimal cutoff identified by the Youden Index was 4 minutes (sensitivity = 0.17, specificity = 0.90). Multivariable logistic regression revealed higher odds of prehospital ROSC in patients aged 18–60 (OR = 3.650), 60–74 (OR = 2.957), and 74–83 (OR = 2.182) compared to the oldest group. ROSC was also more likely when arrests were witnessed (OR = 2.788), initial ECG rhythm was shockable (OR = 3.105), bystander CPR was performed (OR = 1.881), EMS defibrillation was provided (OR = 4.554), and response time met the 4-minute threshold (OR = 2.812).
Conclusion
Shorter emergency medical service response times were associated with improved survival among out-of-hospital cardiac arrest patients. These findings highlight the need for systematic policy measures, including the development of community-based early recognition systems and the optimization of emergency resource allocation to reduce response times.
|
|
|
|