ABSTRACTS
Accessing Higher Levels of CareAuthor: Morgan Anderson MPH | Research Manager | ImageTrend Associate Authors: Powell, Jonathan | Gage, Christopher | Yang, Hannah | Little, Eliza | Vossbrink, Anne | Geissert, Peter | Alvarez, Felicia | Viitanen, Amber | Taylor, Doug Iversen, Lance | Otsby, Jay Pore, Chad
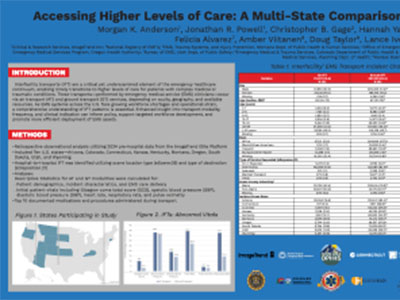
Introduction Interfacility transports (IFT) are a critical yet underexamined element of the emergency medical service (EMS) continuum, enabling timely transitions to higher levels of care for complex etiologies. These transports performed by EMS occur via air transport (AT) and ground transport (GT) services, depending on acuity, geography, and available resources. As EMS systems across the U.S. face increased workforce and operational strain, a comprehensive understanding of IFT patterns is essential. Our objective was to describe the utilization of EMS AT and GT for hospital-to-hospital IFT. Methods We performed a retrospective observational analysis of ten U.S. states in 2024. We identified hospital-to-hospital IFT using scene location and destination types from EMS records using ImageTrend Elite. We used descriptive statistics to compare AT and GT modalities, including patient demographics, incident characteristics, EMS care delivery, and initial patient vitals (e.g., Glasgow coma total score (GCS), systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate(HR), respiratory rate(RR), and pulse oximetry(PO)). Results Of 463,628 IFTs, 72,397 (16%) used AT and 391,231 (84%) used GT. Patient characteristic differences were noted in pediatric ≤1 year (6.3% vs. 3.3%), white race (51.3% vs. 67.7%), missing race (22.4% vs. 9.8%), and non-metro incident location (53.2% vs. 20.7%). AT had a higher proportion of neurological (18.0% vs. 8.7%), cardiovascular (15.7% vs. 9.9%), injury/trauma (10.7% vs. 6.3%), severe GCS (6.0% vs. 1.3%), abnormal SBP (38.0% vs. 35.8%), abnormal DPB (18.9% vs. 13.9%), abnormal HR (39.2% vs 26.9%), abnormal PO (4.1% vs. 3.0%), and abnormal RR (37.7% vs 14.4%) incidents. While scene location and destination type indicated hospital-to-hospital transfers, 7.4% of AT and 12.1% of GT had a service request of 9-1-1 response. This finding may reflect variation in state-level protocol or operational differences. Conclusion Interfacility AT were more commonly associated with higher-acuity cases defined by abnormal vital signs and were more likely to occur in non-metro areas. These patterns highlight the essential role of AT in supporting access to advanced care across geographically dispersed regions and underscore the need for further research into EMS triage, transport decision-making, and interfacility coordination to optimize resource use and ensure equitable patient care.
|