ABSTRACTS
Mitigating Gastric Insufflation in Simulated ResuscitationAuthor: David Olvera MBA, FP-C, NRP, CMTE | Clinical Manager | AirLife Associate Authors: Boone, Otho, BSME | Riccio, Christina, MD
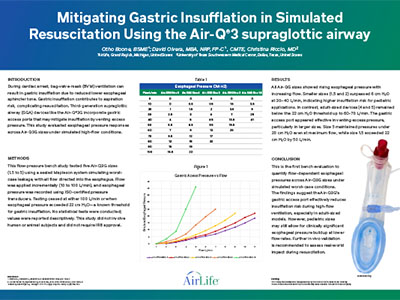
Abstract During cardiac arrest, bag-valve-mask (BVM) ventilation may lead to gastric insufflation due to reduced lower esophageal sphincter tone, increasing the risk of aspiration and complicating resuscitation. Third-generation supraglottic airway (SGA) devices like the Air-Q3G include gastric access ports that may vent excess pressure and reduce insufflation. This bench study evaluated esophageal pressure responses across Air-Q3G sizes under simulated high-flow conditions. Methods Five Air-Q3G sizes (1.5 to 5) were tested using a sealed Mapleson system to simulate worst-case leakage, directing all flow into the esophagus. Flow was incrementally increased (10–100 L/min), and esophageal pressure was recorded via ISO-certified pressure transducers. Testing ended at 100 L/min or when pressure exceeded 22 cm H ₂O—a known threshold for gastric insufflation. Values were reported descriptively. No human or animal subjects were used, and IRB approval was not required. Results All sizes showed increased esophageal pressure with rising flow. Pediatric sizes (1.5 and 2) exceeded 6 cm H ₂O at 30–40 L/min and reached over 22 cm H ₂O by 50 L/min, indicating higher insufflation risk. Adult sizes (4 and 5) stayed below 22 cm H ₂O up to 60–70 L/min. The gastric access port appeared effective in relieving excess pressure, especially in larger sizes. Size 5 remained under 20 cm H ₂O at maximum flow. [IMAGE] Conclusion The Air-Q3G’s gastric access port may reduce insufflation risk under high-flow conditions, particularly in adult sizes. However, pediatric models may still permit significant esophageal pressure buildup. Further in vivo studies are needed to assess clinical relevance.
|