ABSTRACTS
Urgency vs. Outcome: Evaluating the Relationship Between Lights and Sirens Use and Emergency Department DispositionAuthor: John MacMillan | CEO / Educator | Quality Rescue Services Training, LLC Associate Authors: Limmer, Stephanie | Stephen, Rebeka DO | Rollman, Jeffrey | Clemency, Brian DO
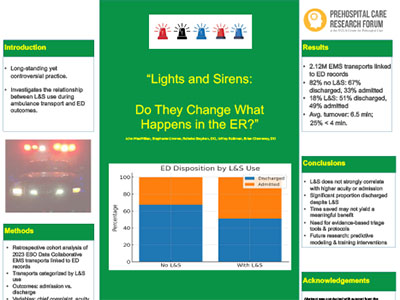
Introduction The use of lights and sirens (L&S) in emergency medical services (EMS) is a long-standing yet controversial practice, traditionally aimed at reducing transport times and improving patient outcomes. However, its clinical necessity and impact on patient disposition remain uncertain. This study investigates the relationship between L&S use during ambulance transport and subsequent emergency department (ED) outcomes, specifically focusing on discharge or admission status. Methods We conducted a retrospective cohort analysis using 2023 ESO Data Collaborative EMS transports and linked ED records. Transports were categorized based on L&S use, and patient outcomes were analyzed based on admission or discharge from the ED. Additional variables such as chief complaints, acuity, prehospital interventions, and EMS-to-ED turnover times were also examined. Results Of the 2.12 million EMS transports linked to ED records, 1.79 million (86.46%) were either discharged to home or self-care or admitted to the hospital. Among these, 1.47 million (82%) were transported without L&S, and 0.3 million (18%) with L&S. Those transported without L&S were discharged in 67.45% of cases and admitted in 32.55%. In contrast, among those transported with L&S, 51% were discharged and 49% admitted. Notably, L&S transports had an average hospital turnover time of 6.5 minutes, with only 25% of handoffs completed within 4 minutes. Conclusion These findings suggest that L&S use often does not correlate with higher acuity requiring urgent admission. A significant proportion of L&S transports were discharged, raising concerns about potential overuse. Moreover, the marginal time saved may not translate into meaningful clinical benefit, especially when weighed against the increased risks to EMS personnel, patients, and the public. These findings underscore the need for better triage tools, clinical decision-making frameworks, and evidence-based protocols to guide the use of L&S. Refining these practices may enhance EMS safety, optimize resource allocation, and maintain quality patient care. Future research should focus on predictive modeling and training interventions that support more appropriate deployment of L&S in prehospital care.
|