ABSTRACTS
Low Acuity, High Activity: EMS Responses to SeniorsAuthor: Scott Bourn PhD, RN | Senior Quality Consultant | ESO Associate Authors: Treichel, Ali, MPH | Colwell, Christopher, ScM | Crowe, Remle P, PhD, NREMT | Green, Alyssa, MS, Paramedic | Fernandez, Antonio, PhD, NRP | Myers, J Brent, MD, MPH
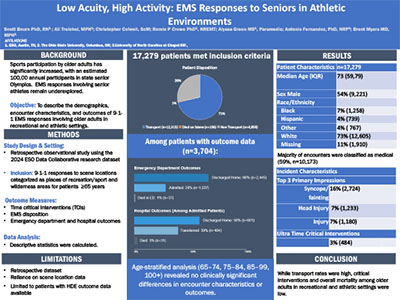
Introduction Since the 1970s there has been a significant increase in sports participation among older adults, with more than 100,000 individuals participating in the US National Senior Games and qualifying events annually. Despite this trend, EMS responses involving senior athletes remain under-explored, particularly around clinical decision-making and patient outcomes. Objective To describe the demographics, encounter characteristics, and outcomes of 9-1-1 EMS responses involving older adults in recreational and athletic settings. Methods This retrospective observational study used data from the ESO Data Collaborative, including all 9-1-1 responses between January 1 and December 31, 2024 to scene locations categorized as places of recreation/sport, recreation areas, or wilderness areas. Patients aged 65-112 were included. Outcomes of interest were time-critical-interventions (TCIs), EMS disposition, and, when available, emergency department (ED) and hospital outcomes. Descriptive statistics were used, including age-stratified analysis. Results Out of 12,568,565 9-1-1 encounters, 17,279 met inclusion criteria. The median patient age was 72 years (IQR 69–79), and 54% were male. Most encounters were classified as medical (58.9%), followed by trauma (35%) and mixed presentations (5%). The most common EMS primary impressions were syncope/fainting (16%), head injury (7%), and general injury (7%). TCIs were rare (3%). Most patients (71%) were transported; 0.6% died on scene. Among the 3,704 patients with ED outcome data, 66% were discharged home, 28% were admitted, and 0.9% died in the ED. Of admitted patients, 58% were discharged home, 3% died, 39% were transferred to another healthcare facility. Age-stratified analysis (65–74, 75–84, 85–99, 100+) revealed no clinically significant differences in encounter characteristics or outcomes. Conclusion Critical interventions and overall mortality among older adults in recreational and athletic settings were low. While the majority of these patients were transported, most were discharged from the ED and did not require hospital admission. Given the growing aging athletic population and lack of prior data, further research is needed to guide EMS protocols and optimize care for this demographic. Limitations include scene location data may not reliably distinguish between participants and bystanders and warrants further investigation.
|