ABSTRACTS
A National Comparison of Outcomes for Prehospital Mechanical versus Manual Ventilation in Medical PatientsAuthor: Melanie Robison | | Associate Authors: Andrea LaLumia MEd NRP, Nichole Berge MPS NRP, Christine O’Neil MEd NRP, Remle Crowe PhD NREMT, Betty Y Yang MD MS
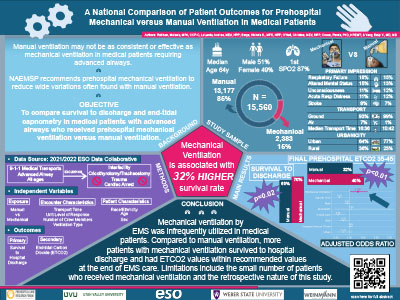
Background: Mechanical ventilation is linked to more consistent, effective respiratory support compared to manual ventilation. However, limited data exist evaluating widespread prehospital practice by ventilation type and few studies have evaluated the association between the ventilation type and outcomes. We aimed to compare survival to discharge and end-tidal capnometry in medical patients with advanced airways who received prehospital mechanical ventilation versus manual ventilation. Methods: We used the 2021-2022 ESO Data Collaborative public use research datasets for this retrospective study. We included all 9-1-1 transports for medical patients of all ages with documented advanced airways. We excluded interfacility transports, patients with cardiac arrest, trauma, existing tracheostomy, and cricothyrotomy. Mortality was derived from hospital discharge disposition. Advanced airway was defined as supraglottic airway (SGA), endotracheal intubation (ETI), and retrograde intubation with at least one successful airway. The exposure was type of ventilation (mechanical vs manual). The primary outcome was survival to hospital discharge, and the secondary outcome was end-tidal carbon dioxide (ETCO2) between 35-45mmHg. Multivariable generalized estimated equations were used to evaluate the association between ventilation type and outcomes, adjusting for age, gender, unit level of care, transport time, urbanicity, and clustering by agency. Results: We analyzed records for 15,560 patient encounters. Of those, 15.3% (2,383/15,560) received mechanical ventilation, and 84.7% (13,177/15,560) received manual ventilation. Among patients with linked hospital data (n=3,106), the survival to hospital discharge rate following advanced airway was 70.1% (356/508) for patients receiving mechanical ventilation and 64.6% (1,677/2,598) for patients receiving manual ventilation, p=0.017. Among patients with ETCO2 values recorded (n=14,604), the goal ETCO2 of 35-45mmHg was achieved for 39.5% (938/2383) for mechanical and 32.1% (3930/13,177) for manual ventilation, p<0.001. Compared to manual ventilation, the adjusted odds of survival to hospital discharge was 32% greater for those receiving mechanical ventilation (aOR:1.32 [1.03-1.69]). Conclusions: Mechanical ventilation by EMS was infrequently utilized in medical patients. Compared to manual ventilation, more patients with mechanical ventilation survived to hospital discharge and had ETCO2 values within recommended values at the end of EMS care. Limitations include the small number of patients who received mechanical ventilation and the retrospective nature of this study.
|