ABSTRACTS
Unhoused Patients and EMS TransportationAuthor: Maya Mullen | | Associate Authors: Em L. Cyr BS NREMT, Denise Whitfield MD, Morgan K.Anderson MPH CPH
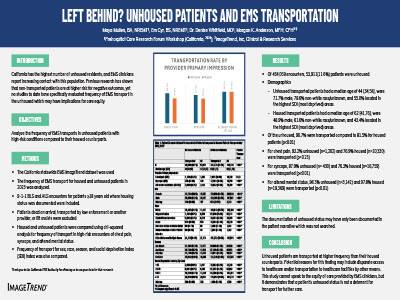
Background: California has the highest number of unhoused residents within the US, and Emergency Medical Service (EMS) clinicians report increasing contact with this population. Previous research has shown that non-transported patients are at higher risk for negative outcomes, yet no studies to date have evaluated frequency of EMS transport in the unhoused, which may have implications for care equity. The objective of this study was to evaluate the frequency of EMS transports in unhoused patients compared to their housed counterparts. Methods: The California EMS ImageTrend dataset was used to analyze the frequency of EMS transport for housed and unhoused patients in 2023. 9-1-1 encounters for patients ≥18 years old where housing status was documented were included. Dead on arrival dispositions, transfers of care on scene and lift-assists were excluded. Housed and unhoused patients were compared using chi-squared analysis for frequency of transport in high-risk encounters of chest pain, syncope, and altered mental status. Frequency of transport for sex, race, season, and social deprivation index (SDI) index was also compared. Results: Of 464,059 encounters, 53,911(11.6%) patients were unhoused. Of the unhoused, 90.7% were transported compared to 81.5% for housed patients (p<0.01). For chest pain, 93.2% (n=1,202) and 76.9% (n=10,330) were transported (p=0.23); for syncope, 87.9% (n= 430) and 76.3% (n=16,759) were transported (p<0.01); for altered mental status, 98.3% (n=3,142) and 97.8% (n=19,369) were transported (p<0.01) for unhoused and housed, respectively. This trend remained across the secondary variables studied. Conclusion: Unhoused patients are transported at higher frequency than their housed counterparts. Potential reasons for this finding may include disparate access to healthcare by other means. This study cannot speak to the equity of care provided, but demonstrates that if there is a disparity in health care for the unhoused, its root cause is not a lack of transport by prehospital providers. Further studies should focus on treatments administered and follow up care for the unhoused.
|