ABSTRACTS
A Statewide Comparison of Prehospital Mechanical and Manual Ventilation for Injured PatientsAuthor: Andrea LaLumia | | Associate Authors: Yukiko Yoneoka MS, Melanie Robison MPA CCP-C, Nichole Berge MPS NRP, Christine O’Neil MEd NRP, Betty Y Yang MD MS, Remle Crowe PhD NREMT
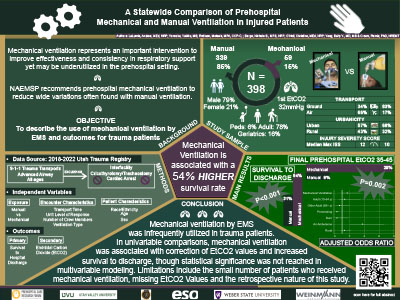
Background: Mechanical ventilation represents an important intervention to improve effectiveness and consistency in respiratory support, yet may be underutilized in the prehospital setting. Limited research has explored prehospital use of mechanical ventilation for trauma patients. Our objective was to describe use of mechanical ventilation by EMS and outcomes for trauma patients using a statewide registry. Methods: We analyzed records from the Utah Trauma Registry with linked prehospital data between 2018 and 2022 for this retrospective study. We included all 9-1-1 encounters where a prehospital advanced airway was placed. Advanced airways included supraglottic airways and endotracheal intubations. Our primary exposure was prehospital manual or mechanical ventilation. Our primary outcome was survival to hospital discharge and the secondary outcome was a final prehospital end-tidal capnography (EtCO2) value of 35-45mmHg. Chi-square tests were used for descriptive outcome comparisons. We used multivariable logistic regression to evaluate the association of ventilation type with survival, adjusting for injury type (blunt, penetrating, burn), age group (pediatric, adult, geriatric), air ambulance transport, and rurality. Results: We analyzed records for 398 patients with prehospital advanced airway and 34% survived to hospital discharge. Prehospital EtCO2 values were recorded for 55% (n=217) of patients. Overall, 15% (n=59) received mechanical ventilation. Of patients receiving prehospital mechanical ventilation, 66% (n=39) were transported by air ambulance. A greater proportion of patients receiving mechanical ventilation survived to discharge, compared to those receiving manual ventilation (54% vs 31%,p<0.001). Among patients with an abnormal initial EtCO2 reading, more mechanically ventilated patients had a normal final EtCO2 reading compared to manually ventilated patients (29% vs 8%,p=0.002). After adjustment, there was not a statistically significant difference in survival for those who were mechanical versus manual ventilation (OR:1.70, 95%CI:0.83-3.50). Conclusions: Mechanical ventilation was used infrequently in the prehospital setting following advanced airway placement among injured patients, particularly among ground EMS crews. In univariable comparisons, mechanical ventilation was associated with correction of EtCO2 values and increased survival to discharge, though statistical significance was not reached in multivariable modeling. Limitations include the small number of patients who received mechanical ventilation, missing EtCO2 values, and the retrospective nature of this study.
|