ABSTRACTS
EMS is Less Accurate at Diagnosing CVAs Among Black, Hispanic, and Socially Vulnerable Populations<p>Misdiagnosis of cerebral vascular accidents (CVAs) by EMS clinicians results in increased risk of injuries, permanent disability, and death. CommunicationAuthor: Nelea Fong | | Associate Authors: Kobe Wright MS NREMT, Tiffany Phan EMTP BS, Claudia Del Toro PA MMS, Bengie Alexandre MS, Yahya Elshawarbi NREMT, Sukai Curtis-Contreras BA EMTP, Jamie Kennel PhD MAS NRP
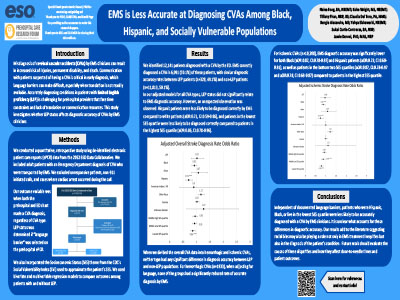
Misdiagnosis of cerebral vascular accidents (CVAs) by EMS clinicians results in increased risk of injuries, permanent disability, and death. Communication with patients suspected of having a CVA is critical in early diagnosis, which language barriers can complicate. Accurately diagnosing prehospital patients with limited English proficiency (LEP) is challenging due to time and resource constraints. This study investigates whether LEP status affects diagnostic accuracy of CVAs by EMS. We conducted a quantitative, retrospective study using de-identified electronic patient care report (ePCR) data from the 2022 ESO Data Collaborative. We included adult patients diagnosed with CVA in the ED that were transported by EMS. We excluded unresponsive patients, non-911 calls, and cardiac arrests. Our outcome variable was the match frequency of CVA diagnosis between prehospital and ED clinicians. LEP status was determined if “language barrier” was selected on the prehospital ePCR. We used bivariate and multivariable regression models to compare outcomes among patients with and without LEP. We identified 12,141 patients diagnosed with CVA by the ED. EMS correctly diagnosed CVA in 6,081 (50.1%) of these patients, with similar diagnostic accuracy rates between LEP patients (n=328, 49.1%) and non-LEP patients (n=11,813, 50.1%). In all our adjusted models for CVA types, LEP status did not significantly relate to EMS diagnostic accuracy. However, Hispanic patients were less likely to be diagnosed correctly by EMS compared to white patients (aOR:0.71, CI:0.59-0.86), and patients in the lowest socioeconomic status (SES) quartile were less likely to be diagnosed correctly compared to patients in the highest SES quartile (aOR:0.86, CI:0.78-0.96). For ischemic CVAs (n=10,208), EMS diagnostic accuracy was significantly lower for Black (aOR:0.87, CI:0.78-0.97) and Hispanic patients (aOR:0.73, CI:0.60-0.91), as well as patients in the lowest two SES quartiles (aOR:0.87, CI:0.78-0.97; aOR:0.78, CI:0.69-0.87) compared to patients in the highest SES quartile. Independent of documented language barriers, patients who were Hispanic, Black, or had fewer socioeconomic resources were less likely to be accurately diagnosed with a CVA by EMS clinicians. It is unclear what accounts for these differences in diagnostic accuracy. Future work should evaluate possible causes of these disparities and whether they affect door-to-needle times and patient outcomes.
|