ABSTRACTS
Validating the Use of RPM Score for Triage of Injured Patients in a Current Trauma PopulationAuthor: Earl V Culvey III | | Associate Authors: Andrew Kuznetsov NRP, George Koshy DO, Shaylin Dalton BA, Antonio R Fernandez PhD NRP FAHA, Douglas F. Kupas MD FAEMS FACEP
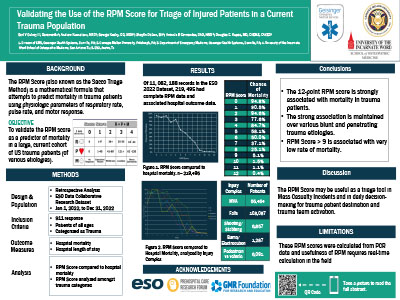
Introduction: The RPM score (also reported as the Sacco Triage Method) is a mathematical formula that attempts to predict mortality in trauma patients using physiologic parameters of respiration, pulse, and motor response. Methods: This retrospective study analyzed prehospital and hospital data from the ESO Data Collaborative from January 1, 2022 to December 31, 2022. This study included all 9-1-1 responses for transported patients that were classified as a trauma by EMS clinicians. The prehospital RPM score was calculated using first available prehospital values for respiratory rate, heart rate, and motor score. RPM is a continuous score ranging from 0-12, with lower scores representing more severe physiologic derangement. The relationship between the patient RPM scores and a disposition of death at the initial destination hospital are reported. Pre-hospital deaths, interfacility transports, and canceled calls were excluded. The primary outcome measure was mortality. Secondary analyses were performed evaluating RPM scores and mortality within subgroups of traumatic mechanisms: motorized vehicle/aircraft accidents, bicycle/pedestrian accidents, shooting/stabbings, and falls. Descriptive statistics were calculated. Results: There were 1,025,414 patients transported in response to 9-1-1 calls with traumatic injury during the study period. Of those, 219,495 (21.4%) had linked hospital outcome data available. The mortality rate associated with each level of RPM score was: 0=94.8%; 1=90.5%, 2=94.6%, 3=77.6%, 4=84.7%, 5=58.2%, 6=50%, 7=37.1%, 8=25.1%, 9=5.1%, 10=1.5%, 11=1.1%, 12=0.4%. Cumulatively, an RPM >9 was associated with a mortality of only 3.1%. RPM was similarly associated with mortality in the subgroups of traumatic mechanisms where an RPM >9 was also associated with a low chance of mortality. Conclusion: The RPM score was strongly associated with mortality in injured patients. This strong association was maintained in sub analyses of various mechanisms of blunt and penetrating trauma, with an RPM score >9 associated with a very low percentage of mortality. RPM may be a useful tool for both mass casualty incident trauma triage and daily decisions regarding individual trauma patient destination and trauma team activation.
|