ABSTRACTS
Prehospital Blood Administration by Ground EMS in North CarolinaAuthor: James E. Winslow, Tom Mitchell, James A. Hood, Joseph Zalkin, Randi Schaefer, Jeff Hinshaw, Mark Piehl, J. Brent Myers, Jennifer K. Wilson, Christopher Montera, and Antonio R. Fernandez | | Associate Authors:
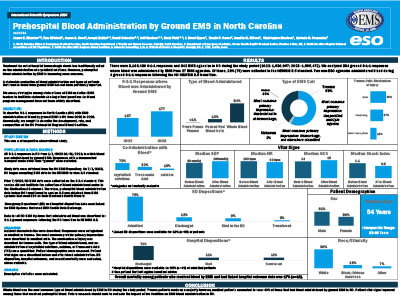
p>Introduction: A statewide evaluation of blood administration during 9-1-1 ground responses and types of patients receiving prehospital blood has not been previously reported. Objective: To describe 9-1-1 ground responses in North Carolina (NC) with EMS administration of blood from 2022 to 2023. Methods: This retrospective study included all NC 9-1-1 responses from January 1, 2022, to December 31, 2024, where blood was administered by ground EMS. Transport modes other than “ground” were excluded. Responses were categorized as trauma or medical. Trauma was categorized by mechanism of injury. The most common provider primary impression was described for medical. For all responses, type of blood administered and coadministration of crystalloids, calcium, or tranexamic acid (TXA) were quantified. Vital signs were described before and after blood administration. Outcomes were described for records from agencies that used the ESO Health Data Exchange. Emergency department (ED) disposition, hospital outcomes, and overall mortality were evaluated, where available. Descriptive statistics were calculated. Results: A total of 334 responses (2022: n = 157; 2023: n = 177) were evaluated. Almost 60% were trauma. Mechanism of injury was 45% blunt, 37% penetrating, and 18% multitrauma/other. The most common medical impression was gastrointestinal hemorrhage (42%). Overall, whole blood (87%) was administered most often, followed by packed red blood cells (13%). Coadministration of crystalloids was documented in 72%, TXA in 32%, and calcium in 15%. Median systolic blood pressure before blood administration was 90 mm Hg (IQR = 72–110) and rose to 100 mm Hg (IQR = 85–117) post-administration. Median pulse pre-administration was 100 BPM (IQR = 79–120) and 95 BPM (IQR = 79–117) post-administration. Median Glasgow Coma Scale pre-administration was 14 (IQR = 6–15) and 15 (IQR = 8–15) post administration. Median shock index was 1.1 (IQR = 0.8–1.4) pre administration and 0.9 (IQR = 0.8–1.2) post administration. Linked outcomes were available for 18%. Of those, 76% were admitted, 12% discharged, 9% died in the ED, and 3% transferred. Hospital dispositions were available for 95% of admitted patients. Of those, 71% were discharged, 12% transferred, and 12% died. Overall mortality among records with linked outcomes was 17%. Conclusion: Whole blood was the most common type of blood product administered. Trauma patients received blood most often; however, medical patients accounted for over 40%. Vital signs improved following blood administration.
|