Racial and Ethnic Minorities Are Less Likely to Be Transported by EMS: A National Investigation into Abdominal and Chest Pain Complaint
Author: Abraham Pritzker, Anagha Rajesh, Hunter Gregg, Penny K. Engelking, Dawn Bloemer, and Jamie Kennel | |
Associate Authors:
<p><strong>Introduction:</strong></p>
<p>Patients who request emergency medical services (EMS) but are not transported represent a medical risk to patients and a legal risk to the EMS agency. Although racialized patients are known to receive substandard care from EMS clinicians, it is unclear whether they are also at greater risk of not being transported. Better understanding racial differences in EMS nontransport rates is critical to improving EMS agency operations as well as health disparities.</p>
<p><strong>Objective:</strong></p>
<p>To investigate the association between race and nontransport for patients with abdominal or chest pain.</p>
<p><strong>Methods:</strong></p>
<p>A cross-sectional, retrospective, observational study using the 2022 ESO Data Collaborative was conducted. Two patient conditions were included: (1) a primary impression of atraumatic abdominal pain and (2) cardiac chest pain that was not a STEMI. Bivariate and multivariable logistic regression models were used to compare nontransport rates by race.</p>
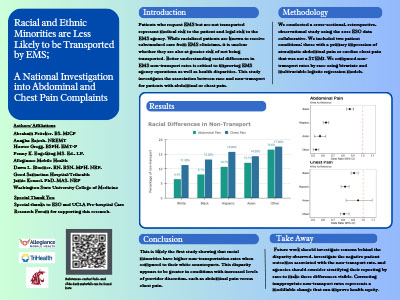
<p><strong>Results:</strong></p>
<p>Of the sample of 744,124 patients, the nontransport rate was 9.2%, and all racialized patients had higher nontransport rates. In the multivariable model adjusted for demographic and clinical characteristics, Black (aOR = 0.93, 95% CI = 0.91–0.96), Hispanic (aOR = 0.76, 95% CI = 0.73–0.79), and Asian (aOR = 0.75, 95% CI = 0.69–0.70) patients are all less likely to be transported compared to their White counterparts. This disparity was seen for Black (aOR = 0.91, 95% CI = 0.88–0.95) and Hispanic (aOR = 0.82, 95% CI = 0.78–0.86) patients with chest pain and increased in Black (aOR = 0.87, 95% CI = 0.84–0.91), Hispanic (aOR = 0.63, 95% CI = 0.60–0.66), and Asian (aOR = 0.57, 95% CI = 0.51–0.63) patients with abdominal pain.</p>
<p><strong>Conclusion:</strong></p>
<p>This is likely the first study showing that racial minorities have higher nontransportation rates compared to their White counterparts. This disparity appears to be greater in conditions with increased levels of provider discretion, such as abdominal pain versus chest pain. Future work should investigate reasons behind the disparity observed, and agencies should consider stratifying their reporting by race to make these differences visible. Correcting inappropriate nontransport rates represents a modifiable change that can improve health equity.</p>
|
|
|
|