ABSTRACTS
First-Touch Treatment for Out-of-Hospital Cardiac Arrest Patient Prognostic Comparison Using Propensity Score Matching Between Shock First and CPR FirstAuthor: Ryu Kimura, Koshi Nakagawa, Tomoya Kinoshi, and Hideharu Tanaka | | Associate Authors:
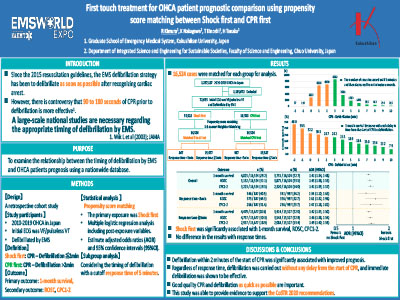
Introduction: Defibrillation of out-of-hospital cardiac arrest (OHCA) with shockable rhythm by emergency medical technicians (EMTs) as soon as possible has been a standard strategy worldwide since the 2005 resuscitation guidelines. However, debate continues whether waiting 90 to 180 seconds before initiation of defibrillation by emergency medical services (EMS) is effective. There is also insufficient evidence from large observational studies of the association between defibrillation within 2 minutes after initiation of CPR (shock first) or after 2 minutes (CPR first) and outcome following OHCA. Objective: To examine the association between the timing of first defibrillation by EMT and outcome after OHCA. Methods: The study included 71,088 patients aged 15 years or older with nontraumatic OHCA whose initial rhythm was ventricular fibrillation or pulseless ventricular tachycardia and who underwent EMT defibrillation in Japan between 2010 and 2019, recorded in Utstein style. Patients were divided into two groups, the shock-first group, in which defibrillation was performed within 2 minutes of CPR initiation, and CPR-first group, in which defibrillation was performed after 2 minutes. The primary outcome was 1-month survival; secondary outcomes were return of spontaneous circulation (ROSC) and good brain function (CPC1-2). The primary outcome was shock, with 1:1 propensity score matching. Multiple logistic regression analysis was performed to estimate adjusted odds ratios (aOR) and 95% confidence intervals (95% CI) for the association between exposure and outcome. Results: After propensity score matching, there were 16,266 cases in each group. The 1-month survival was 29.7% in the shock-first group versus 22.8% in the CPR-first group. The shock-first group showed a significant positive association with 1-month survival (aOR = 1.43, 95% CI = 1.36–1.51). Similarly, a significant positive association was also shown between ROSC and CPC1-2 before hospital arrival (aOR = 1.57, 95% CI = 1.49–1.65 and aOR = 1.53, 95% CI = 1.44–1.63, respectively). Conclusion: Regarding the timing of EMS defibrillation in patients with cardiac arrest, defibrillation within 2 minutes after initiation of CPR was associated with better outcomes. These results support the recommendations of CoSTR2020 and suggest that it is important to provide good-quality CPR until defibrillation is performed while implementing rapid defibrillation team activities.
|